(The petition is at the bottom of this page.)
Diagnostic errors affect millions annually, causing harm, suffering, and even death. Current one-sided internal note systems often hinder patients from promptly disputing erroneous diagnoses, perpetuating mistakes, and jeopardizing lives. Our petition proposes reform.
Key Points:
1. Frequency and Severity: Diagnostic errors account for approximately 10% of patient deaths and 17% of adverse events in hospitals. Many of these errors can be avoided with better communication between the medical professionals and the patients. Our proposed note system will help protect patients the way they deserve to be protected.
2. Delayed Resolution Harms Patients: Prolonged dispute processes exacerbate physical and emotional suffering, reduce trust in healthcare providers, and increase mortality risks. Our proposed note system will provide ample communication between the patient and medical professionals. This way, patients can focus their time on healing and treatment and not on making phone calls to fix errors and request addendums, only to be tossed around in the phone tree and oftentimes not making progress.
3. Current System Failures:
– Lengthy and archaic appeal processes
– Limited patient awareness of rights
– Inadequate provider feedback mechanisms
– Fear of retaliation against whistleblowing patients/providers
4. Benefits of Prompt Dispute Resolution:
– Improved patient safety and outcomes
– Enhanced trust between patients and providers
– Increased transparency and accountability
– Reduced medical errors and malpractice claims
5. Proposed Solutions:
– Establish clear, patient-friendly dispute resolution protocols
– Mandate provider notification of patients’ right to dispute diagnoses
– Create independent review boards for prompt resolution
– Form a culture encouraging open communication and error reporting
Dear PMRA Community,
Let’s revolutionize patient care transparency!
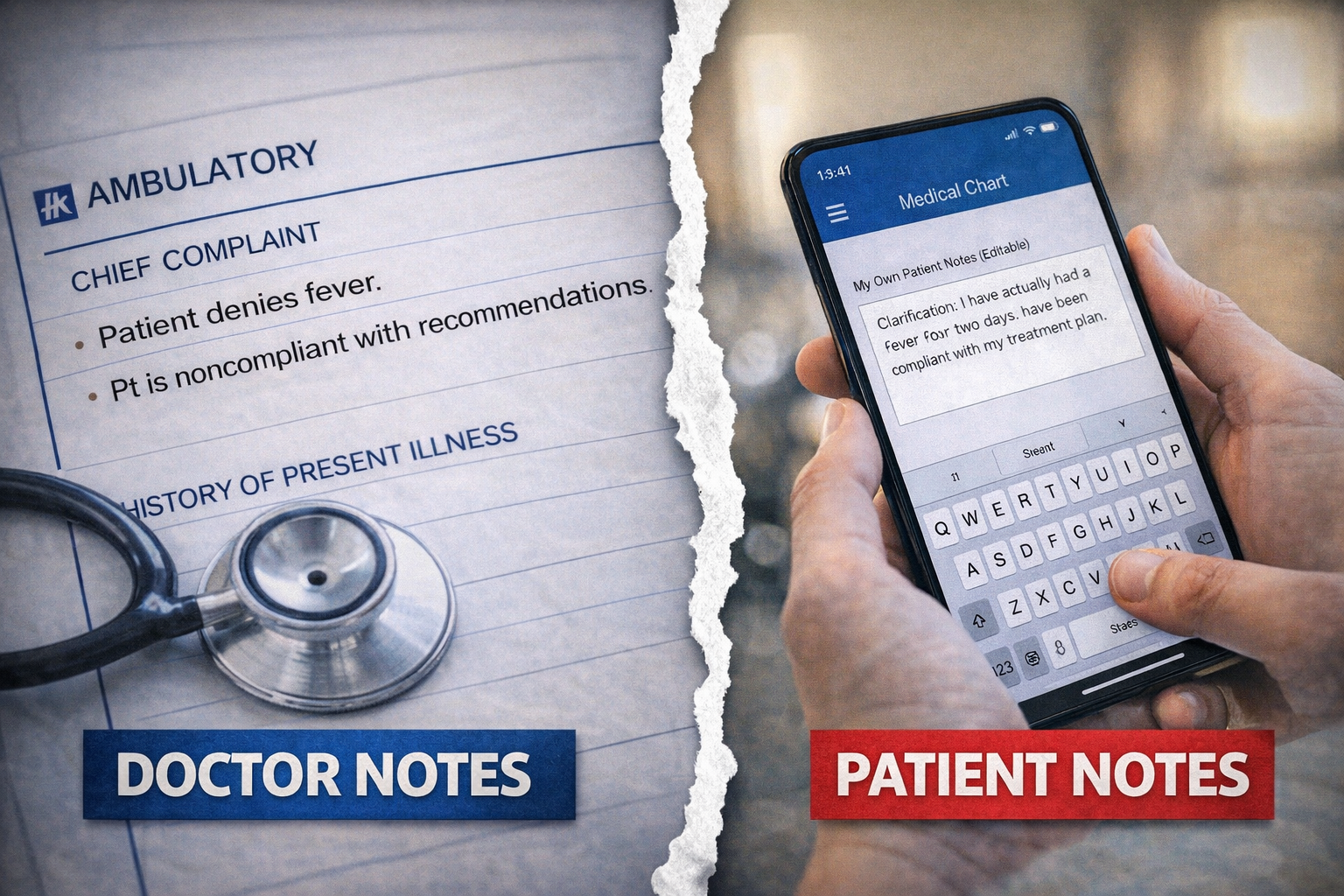
We propose a game-changing solution, a dual-documentation system:
■Patients record their own notes in real-time during (or after) doctor visits, hospital stays, or urgent care trips
■Doctors simultaneously document their own notes — this way transparency is increased!
This initiative aims to:
■Enhance accuracy and reduce miscommunication
■Increase patient engagement and empowerment
■Foster accountability among healthcare providers
■Reduce the amount of medical note errors that could potentially follow patients for years, passing down false info to future doctors, which leads to even more errors
Objective: Petition lawmakers to mandate dual-documentation systems in US healthcare facilities.
Action Plan:
■Survey Support: Please sign our petition below if you support this endeavor and want change! At the bottom comment field, you can even share your thoughts on how dual-documentation would improve patients’ healthcare experiences.
■Influencer Outreach: Collaborate with healthcare advocates, patient rights groups, and social media influencers to amplify our message.
■Legislative Presentation: We intend to deliver petition signatures and collective voice to US lawmakers, demanding dual-documentation system adoption.
Fine details:
PMRA proposes a new or changed medical system initiative that gives patients back their voice — to allow them to write their own medical notes in a mutual note system. The notes can be added straight through an online charting portal (i.e: MyChart), if one exists through the health network.
The current medical system allows medical staff to enter notes at the emergency room of a hospital, as inpatient in a hospital, and at doctors’ offices. However, patients do not currently have this benefit, and this poses the question of fairness. The lack of patients’ voice means the medical networks hold all of the power behind the documenting of care, and patients have to fight very hard to be heard properly. The miscommunications are then passed down to future care teams, creating a perpetual cycle of errors, miscommunications, and medical mishaps. Patients should have the ability to write their own notes as well — not only to respond to the doctors’/nurses’ notes but also to make corrections or even request addendums. Oftentimes, the staff at hospitals are too busy to enter notes live-time, which is understandable, but their notes will appear eventually. Regardless of when the doctors’/nurses’ notes appear in the system, the patient should have the ability to write notes as to why they are at the ER (their reason for the visit), in live-time if possible and afterwards as well. In our proposal, though, if notes are to appear after a hospital visit, the patient should be allowed to wait for the notes to be uploaded into the chart. We push for faster notes in the system when in an emergency situation in the ER as well as when admitted to the hospital. These notes could include details as to specifically what is wrong, symptoms the patient is facing, circumstances, and even medical history, no matter how complex. Patient notes should be allowed to add comments to correct their weight, height, circumstances, and even provide their own story as to why they are being seen. This proposed note system shall not cap the patients’ word count and will allow as many characters as needed. (This should not bog down the systems, as text itself does not take up a lot of data space.) These notes are for protection of both the medical staff and the patients. This way, everyone is protected more (to some degree). The current system is highly unfair and paints a one-sided narrative, as it only allows medical workers to write notes, which leads to mistranslations, miscommunications, errors, and a future of medical note mix-ups that can actually follow a patient for life.
Photos will be allowed as well, but this will need to be capped to 10 photos per visit, to save data space.
When I took a poll from the general public of the accuracy of the notes in their recent hospital stays (for those who had to visit the ER), 95% said there were errors. Most reported errors with even why they were being seen. This comes down to everything from communication with EMS (if applicable), triage (if applicable), doctors, nurses, and techs. Having errors is understandable; however, for this reason, patients should have the ability to correct these errors or at least enter their own remarks / rebuttals. Or, they may even agree with the doctors and nurses with their notes and would like to voice their agreement.
Notes will be able to be entered even after the ER / hospital / doctor / urgent care visit.
If a care team member adds or updates notes, the patient will get an email and/or text alert. If a patient adds or updates notes, the care team members will get alerted through their own alerting system.
The notes will be able to be edited, but then it would show a paper trail of previous notes and will appear with the word “edit” at the top.
The patients may write a note to their doctor in the portal as well.
Collaboration between the medical professional(s) and the patient should be permitted to be documented. If discrepancies between notes exist, the patient should not only have the option to add a note but to also “request an addendum” (or request an edit to the medical professionals’ notes). If the medical professional disagrees, he or she can explain why or why not. These notes do not mean that the patient and medical professional must agree with each other, of course. These notes simply mean that both sides of the story are painted. In the current medical system, 95% of patients report that errors exist on their notes as to even what their symptoms are, what exactly happened at the medical appointment, etc. These inaccuracies lead to a future of confusion when future doctors look at their notes.
For random example, I recently went to the hospital, and the doctor ordered me Tylenol. The nurse walked away in a huff and puff because I had to get another nurse to take my labs, so she forgot to give me the Tylenol. However, my notes still stated that I was given Tylenol, when I was not. The nurses who took over her (as I had to get a new nurse, as she called me a “whack job”) did not realize that I was given Tylenol. That was a small mix-up, but mix-ups like this exist on a higher scale all the time. And, of course, nothing was noted in my chart that the nurse called me names and belittled me. I should have been allowed to document this. The staff gets away with all sorts of things and misconduct all because we as patients are not permitted to note our side of what happened. Many of us get mislabeled as mentally ill due to a trail of incorrect notes. Sometimes, my chart will even say I had a test done that I did not have done. Sometimes it will say I said something that I did not say, or what I say is taken out of context. This is understandable, as people are busy, and miscommunications happen frequently. However, we should be able to clarify ourselves and our words. We should have a voice. “A stitch in 9 saves time.” If we do it the right way from the get-go, we will save more time in the long run.
Hospital patients under this proposal will be legally entitled to stay in their hospital bed until notes are uploaded to their chart and until they have reasonable time to read and reply to the notes.
To sign this petition, please see below!
Proposal for Dual Note System for Both Patients and Medical Professionals
| 22 | Ms. Deirdre H. | Mar 06, 2026 |
| 21 | Ms. A S. | Jan 12, 2026 |
| 20 | Ms. Linda S. | Jan 12, 2026 |
| 19 | Mr. M R. | Jan 12, 2026 |
| 18 | Ms. Ollie S. | Jan 12, 2026 |
| 17 | Ms. Andrea S. | Jan 12, 2026 |
| 16 | Anonymous | Jan 08, 2026 |
| 15 | Anonymous | Jan 07, 2026 |
| 14 | Ms. Amy B. | Dec 14, 2025 |
| 13 | Anonymous | Jul 21, 2025 |
| 12 | Mr. Mark S. | Jul 16, 2025 |
| 11 | Anonymous | Jul 15, 2025 |
| 10 | Ms. Amy B. | Jul 15, 2025 |
| 9 | Mrs. Anna C. | May 01, 2025 |
| 8 | Ms. Elaine S. | Apr 14, 2025 |
| 7 | Anonymous | Apr 14, 2025 |
| 6 | Mr. John B. | Apr 14, 2025 |
| 5 | Anonymous | Apr 14, 2025 |
| 4 | Anonymous | Apr 14, 2025 |
| 3 | Anonymous | Apr 14, 2025 |
| 2 | Anonymous | Apr 14, 2025 |
| 1 | Mr. Daniel R. | Apr 14, 2025 |
Leave a Reply